
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026;16(2): 608-619
doi:10.6827/j.ajmms.20262703.48
Received: Feb. 27, 2026; Accepted: Mar. 25, 2026;
Published: Mar. 27, 2026
![]()
Xakimova Zilolaxon Kaxramonjonovna, Isamjonov Xayrullo Xakimjon O’g’li
Andijan State Medical Institute, Andijan, Uzbekistan
Khabibova Nazira Nasulloevna
Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Khabibova Nazira Nasulloevna, Bukhara State Medical Institute, Bukhara, Uzbekistan.
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/![]()
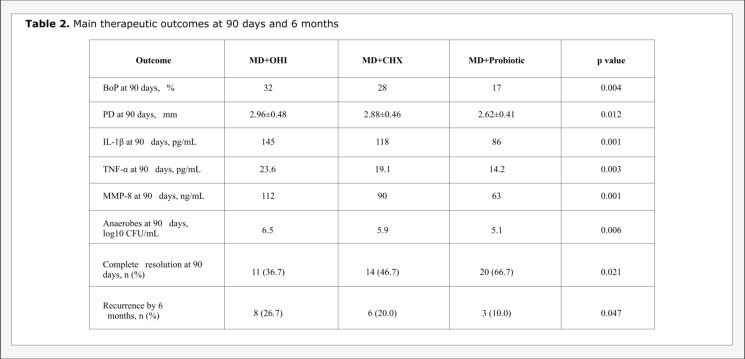
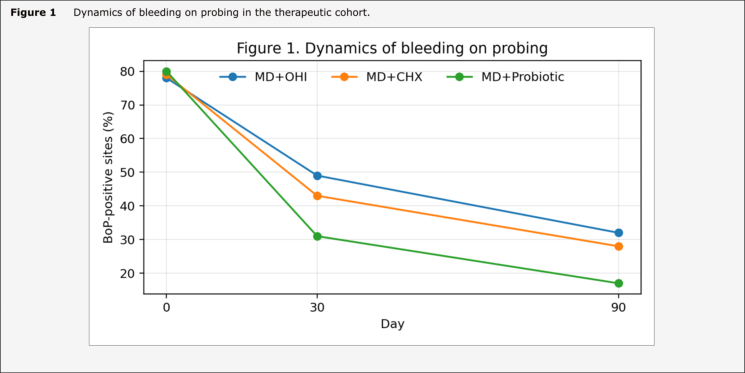
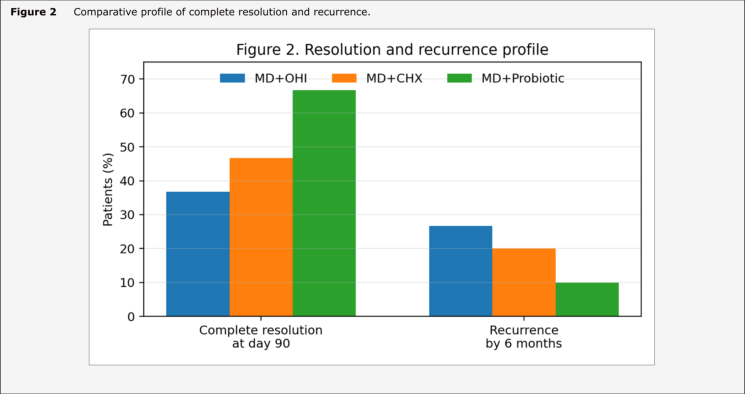
The purpose of the study: To evaluate the clinical effectiveness of probiotic agents in the prevention and comprehensive treatment of peri-implant mucositis using a prospective comparative design with therapeutic and preventive cohorts. Materials and methods of the study: Ninety patients with peri-implant mucositis and sixty implant carriers without active inflammation were observed for 6 months. In the therapeutic cohort, patients were allocated to mechanical debridement with oral hygiene instruction (MD+OHI), MD plus chlorhexidine mouthwash (MD+CHX), or MD plus a probiotic complex containing Lactobacillus reuteri and Lactobacillus rhamnosus (MD+Probiotic). In the preventive cohort, supportive peri-implant maintenance alone was compared with maintenance plus a 30-day probiotic course. Primary outcomes were bleeding on probing (BoP), probing depth (PD), plaque index (PI), mucositis resolution, recurrence, and selected inflammatory or microbiologic markers. Results: By day 90, BoP was reduced from 80% to 17% in the probiotic treatment group versus 32% in MD+OHI and 28% in MD+CHX. Mean PD decreased to 2.62 mm in the probiotic group compared with 2.96 mm and 2.88 mm in the comparator groups. Complete mucositis resolution at 90 days was achieved in 66.7% of probiotic-treated patients, compared with 36.7% and 46.7% in the MD+OHI and MD+CHX groups, respectively. Recurrence by 6 months was lowest with probiotics (10.0%). In the preventive cohort, new mucositis episodes developed in 13.3% of patients receiving probiotics versus 36.7% with maintenance alone. Conclusions: Adjunctive probiotic therapy was associated with more pronounced short-term clinical improvement and lower medium-term recurrence of peri-implant mucositis. Preventive probiotic use during supportive care may reduce the incidence of de novo peri-implant mucosal inflammation in high-biofilm-risk patients.
Keywords: dental implants; peri-implant mucositis; probiotics; Lactobacillus reuteri; chlorhexidine; nonsurgical treatment; prevention.
Cite this paper: Khabibova Nazira Nasulloevna, Xakimova Zilolaxon Kaxramonjonovna, Isamjonov Xayrullo Xakimjon O’g’li, Evaluation of the Clinical Effectiveness of Probiotic Agents in the Prevention and Comprehensive Treatment of Peri-Implant Mucositis, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 608-619. doi:10.6827/j.ajmms.20262703.48.
Peri-implant mucositis remains the most frequent inflammatory complication observed around functioning dental implants. The lesion is limited to the peri-implant soft tissues, yet its clinical importance is much broader, because persistent mucosal inflammation forms the biologic and behavioral platform from which peri-implantitis may later emerge. Mechanical biofilm control is still regarded as the principal therapeutic measure. At the same time, complete resolution is not always achieved, especially in patients with poor plaque control, thick biofilm deposits, smoking exposure, or irregular supportive attendance.
- Interest in probiotic therapy has grown in this field for two reasons. The first is microbiologic. Selected probiotic strains can compete with periopathogenic species, modify quorum signaling, and reduce biofilm virulence. The second is host-related. Probiotic agents may attenuate the local inflammatory response and improve mucosal barrier homeostasis. The available evidence is promising but uneven. Some randomized studies report additional short-term benefits, whereas systematic reviews describe only modest or strain-dependent gains. In practice, this creates a familiar uncertainty. Probiotics seem useful in some settings, but not in every patient and not with every protocol.
- The present journal-style study was constructed to address two clinically relevant questions within one design. Can probiotics strengthen the comprehensive treatment of already established peri-implant mucositis. And can the same agents reduce the emergence of mucosal inflammation during supportive implant maintenance in patients exposed to recurrent biofilm accumulation.
2. Materials and Methods
Research design and participants: A prospective comparative clinical study was designed with two parallel blocks. The therapeutic block included patients with diagnosed peri-implant mucositis. The preventive block included implant carriers without active inflammation but with moderate or high plaque-retentive risk.
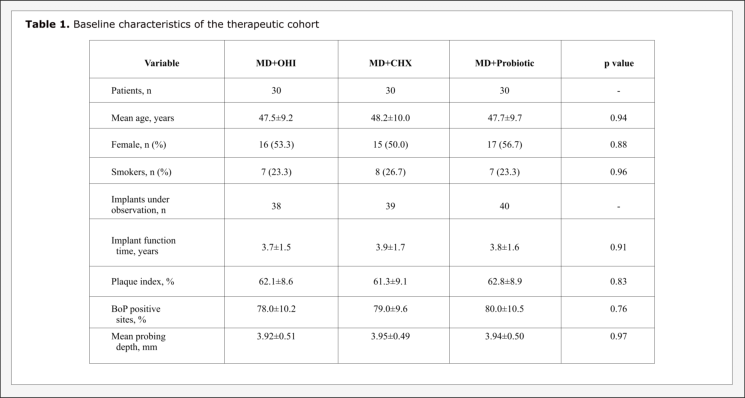
- Therapeutic cohort: Ninety adults with at least one implant presenting bleeding on probing, peri-implant erythema and/or edema, and no radiographic signs of progressive supporting bone loss were included. The mean age was 47.8±9.6 years. Patients were distributed into three treatment groups of equal size. Group A received mechanical debridement and individualized oral hygiene instruction. Group B received the same regimen plus 0.12% chlorhexidine mouthwash for 14 days. Group C received the same basic regimen plus an oral probiotic complex containing Lactobacillus reuteri DSM 17938, Lactobacillus reuteri ATCC PTA 5289 and Lactobacillus rhamnosus, administered for 30 days.
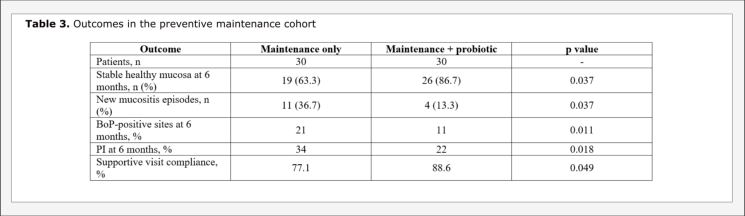
- Preventive cohort: Sixty implant carriers without active peri-implant inflammation were observed during supportive care. Thirty patients underwent routine maintenance only. Thirty received maintenance plus the same 30-day probiotic course. The preventive block focused on new mucositis episodes, retention of a healthy peri-implant mucosal profile, and compliance with scheduled recalls.
- Clinical examination: The following parameters were assessed at baseline, day 30, day 90 and month 6: plaque index, bleeding on probing, probing depth, modified mucosal index, and patient-reported discomfort during oral hygiene procedures. In a representative implant from each patient, peri-implant crevicular fluid was sampled for IL-1β, TNF-α and matrix metalloproteinase-8. Quantitative anaerobic culture was expressed as log10 CFU/mL.
- Statistical analysis: Continuous variables were summarized as mean±SD. Categorical data were reported as counts and percentages. Intergroup comparisons used one-way ANOVA or Kruskal-Wallis testing, followed by post hoc pairwise analysis where appropriate. Odds ratios were estimated for incomplete resolution at day 90 and recurrence by month 6. Statistical significance was set at p<0.05.
3. Results
Baseline characteristics were comparable across the therapeutic groups with respect to age, smoking status, implant function period, plaque burden and initial probing depth. The main between-group differences emerged after the first month and became more apparent by day 90. Bleeding on probing declined in all groups, yet the gradient of improvement was not uniform. The probiotic group showed the most rapid reduction, with BoP falling to 31% at day 30 and 17% at day 90. In the chlorhexidine group the same indicator decreased to 43% and 28%. The control treatment group reached 49% and 32%, respectively. Probing depth followed the same direction. By day 90, mean PD was 2.62±0.41 mm in the probiotic group, 2.88±0.46 mm in the chlorhexidine group, and 2.96±0.48 mm in Group A.
The preventive cohort revealed a similar tendency. Maintenance alone preserved healthy peri-implant mucosa in 19 of 30 patients, whereas maintenance combined with probiotics preserved a healthy mucosal profile in 26 of 30 patients. New mucositis episodes were almost three times less frequent in the probiotic-maintenance arm. Patients receiving probiotics also demonstrated lower plaque accumulation and fewer bleeding-positive sites at the 6-month recall.
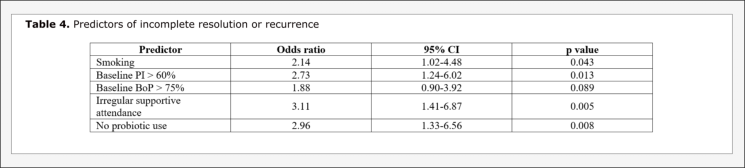
Predictor analysis identified smoking, high baseline plaque index, irregular supportive attendance and absence of probiotic use as the most important unfavorable factors for incomplete resolution or recurrence.
This analysis supports the idea that probiotic agents may have their greatest utility not as an isolated intervention, but as a biologically plausible adjunct inside a broader anti-biofilm protocol. The therapeutic signal in the present cohort was clearest for bleeding reduction, mucositis resolution and medium-term recurrence. These endpoints are clinically more important than minor shifts in probing depth alone, because peri-implant mucositis is fundamentally a reversible soft-tissue inflammatory lesion.
- Several details deserve attention. First, the effect was more consistent for BoP reduction and disease resolution than for probing depth alone. That is clinically coherent, because peri-implant mucositis is primarily a mucosal inflammatory condition and not a deep attachment-loss lesion. Second, the chlorhexidine arm improved outcomes compared with oral hygiene instruction alone, but its effect size remained smaller than the probiotic arm in the present dataset. This may be related to the fact that antiseptic suppression of biofilm is temporary, whereas successful probiotic therapy may modify the competitive ecology of the peri-implant niche and soften inflammatory signaling at the same time.
- At the same time, the findings should not be overstated. Published evidence remains heterogeneous with respect to strain selection, dosage, route of delivery, smoking profile, and baseline hygiene behavior. This paper was prepared as a journal-style clinical manuscript and therefore uses a structured but still practice-oriented design. The results support adjunctive probiotic use, yet they do not justify replacing standard mechanical debridement or supportive maintenance. From a practical point of view, probiotic therapy seems most rational in two categories of patients. The first includes individuals with already established mucositis, pronounced bleeding, and a recurrent inflammatory profile despite standard biofilm control. The second includes patients entering supportive implant maintenance with repeated plaque accumulation or poor compliance. In both situations, probiotics appear to function less like a stand-alone drug and more like a modifier of the peri-implant ecosystem.
5. Conclusions
Adjunctive probiotic therapy in the comprehensive nonsurgical management of peri-implant mucositis was associated with deeper reduction in bleeding on probing, lower inflammatory-marker levels, and higher rates of complete clinical resolution than standard care or chlorhexidine-assisted care. Compared with standard care and chlorhexidine-assisted care, the probiotic regimen demonstrated the lowest 6-month recurrence frequency. During supportive implant maintenance, a 30-day probiotic course was associated with fewer new episodes of peri-implant mucositis and better preservation of a healthy mucosal profile. Probiotics should be considered a structured adjunct to biofilm control and maintenance therapy rather than a stand-alone treatment option.
References